
Managing your health and maintaining a healthy weight
Sudi Narasimhan explores the linkages between obesity, diet and wellness, as part of a series of articles exploring this topic
As the global obesity epidemic continues to sweep both the developed and developing world, people everywhere are desperate for answers. Several decades in the making, we are now more aware of the problem than ever, but recommendations on how to address it are too often varied, divergent, and changing. It has been my personal passion to learn as much as I can in this area to better manage my own health over the course of my lifetime.
It might be helpful to first define what is meant by “obese.” Body type classification is normally done using BMI or body mass index. A dimensionless number, BMI is a ratio of weight (in kg) divided by height (in metres) squared. A BMI less than 18.5 is considered underweight, a range of 18.5 – 25 is considered normal weight, 25 – 30 is classified as overweight, while 30 – 40 is considered obese. A BMI above 40 is classified as morbidly obese and significantly increases a number of associated health risks.
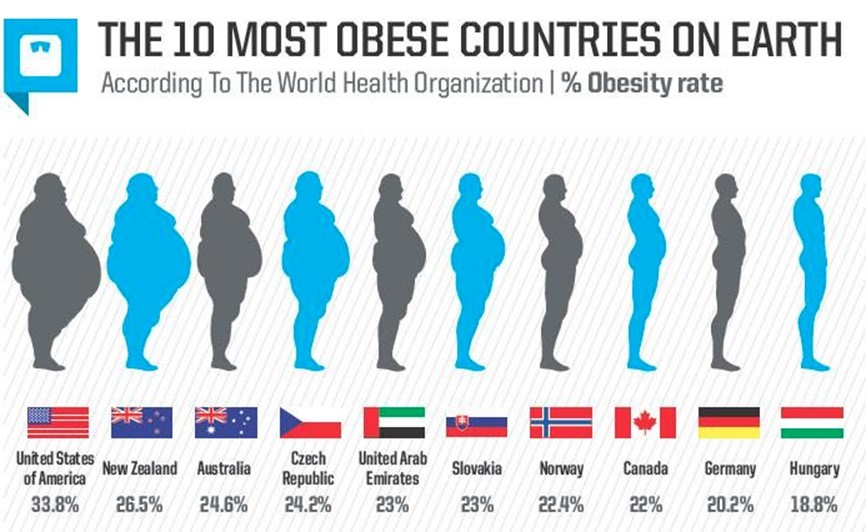
Figure 1: Countries with the greatest number of obese residents, with the percentage of people listed with BMI levels over 30. Source: http://blog.praguemorning.cz/the-10-most-obese-countries-on-earth-czech-republic-ranked-4th/
As can be observed from Figure 1, the US leads the world in obesity with more than a third of the population being classified in this category. New Zealand, Australia, the U.A.E., and many European countries, however, are not far behind.
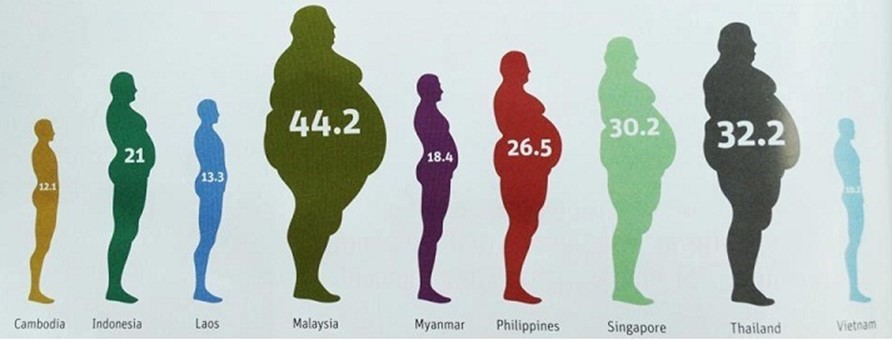
Figure 2: Asian countries showing the number of overweight residents, with the percentage of people listed with BMI levels over 25. Source: http://easicircle.blogspot.ae/2014/06/what-causes-obesity.html
People living in East and Southeast Asian countries have historically been generally smaller and slimmer than their Western counterparts but have been catching up in recent years. Figure 2 shows that Malaysia, Thailand and Singapore have a growing percentage of residents classified as overweight, with a BMI greater than 25. These societies are also quickly aging as the median age increases and population growth slows, a combination that raises medical costs for the entire population.
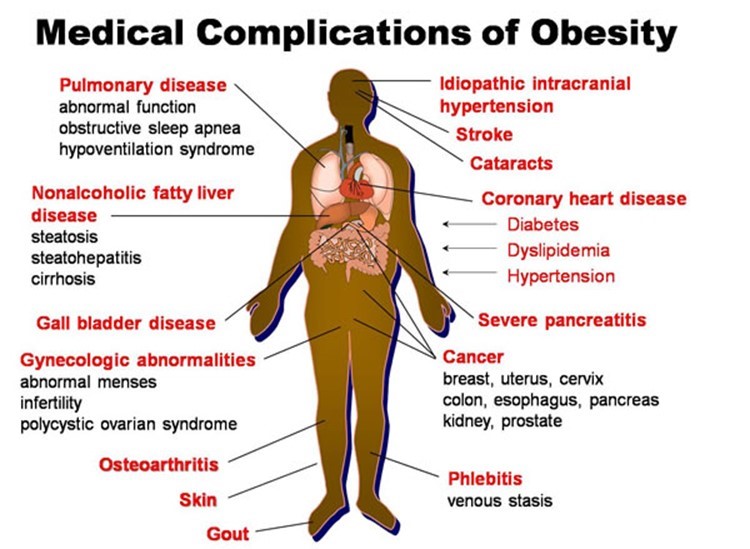
Figure 3: Increased weight is correlated with different health problems. Source: http://www.asyouage.com/19_Medical_Complications_of_Obesity.html
The main causes of death today are heart disease and cancer, although this can vary across countries. Risks for many diseases increase with the addition of extra weight and tend to heighten as we get older. This not only affects our health but also our quality of life, as carrying extra weight is correlated with osteoarthritis, sleep apnea, and impaired liver function. In general, we tend to feel more uncomfortable and are slower to heal and recover from injury or stress.

Figure 4: Obesity is linked or correlated with many disease that impact our quality of life. Source: https://fenfuro.com/about-obesity/
In some cases, being overweight can cause diseases that significantly shorten our life, such as cancer. In others, we are able to manage the disease as a chronic condition but need to take higher doses of different medications over the remainder of our life. Quality of life often suffers in the process as many medications have potent side effects, and the underlying root cause of the disease is not always addressed.
The role of diet in weight management
Gaining or losing weight is simply driven by the number of calories that are consumed relative to the number of calories that are burned over the course of the day. So it is only logical to prescribe that the best way to lose weight is to consume fewer calories than your body needs. That is fairly obvious, but the reality is that this is far easier said than done.
Consider how difficult the challenge is to count every calorie ingested compared to the daily required level of energy consumption. Even overeating by 30 kilocalories (a few crisps) each day would result in a 900 Kcal surplus over one month or more than 10,000 Kcal each year. This would equate to a weight gain of 1.5 kg of body fat each year or 15 kg over a decade. And that is just from a negligible level of overeating each day. Clearly there is more to it than just counting calories.
The role of hunger
It turns out that our bodies are quite effective at maintaining a given weight. This is sometimes referred to as a “set point” where the body fights to sustain a given weight whether a person overeats or under eats on a given day.
Our body’s hunger mechanism is a trigger for signaling a meal or the motivation to seek out food. It is also linked to our habits. Sometimes we may eat when we actually feel thirsty, bored or stressed, as opposed to being genuinely hungry. Interestingly enough, some of the foods we consume can make us hungrier soon after eating. We may not pay attention to this and continue eating them without realizing they are signaling us to feel increased hunger. How many times do we look back on our day and think that we hardly ate at all and wonder why we aren’t able to shed the extra weight that we are carrying?
The dual energy pathway
Our bodies and cells are extremely adaptable to the many different conditions found on planet Earth. We are able to survive and even thrive in tropical climates where fruits are abundant year round. Yet we are also able to survive in polar climates where growing seasons are extremely short and the population’s survival is linked to the success of animal husbandry or hunting as the main source of food.
This is because our cells are able to use two sources of energy for food. The first pathway is glycolysis, which comes from the burning of glucose. All carbohydrates that are consumed are broken down into glucose by the liver and stomach, which is then released into the blood stream to be used by our brain and muscles. We are able to store nearly 1000 Kcal or 250 grammes of glucose (each gramme of carbohydrate is 4 Kcal) in our muscles and liver to be used for energy. Once these stores are full then excess glucose in the blood is sequestered by insulin produced in our pancreas, and this excess glucose is turned into fatty adipose tissue for later storage.
The other energy pathway available to us is ketosis, or the burning of ketones from fat cells through a process known as beta-oxidation. Our muscles, organs, and brain are able to use ketones as a source of fuel and burn the fat that is stored in our bodies and from what is ingested.
To achieve ketosis, our carbohydrate stores need to be depleted. Biochemically, our cells cannot initiate the beta-oxidation process as long as there is elevated insulin caused by ingested glucose levels that are present in our blood stream. The required hormones and enzymes needed to open up the cell walls to admit the fatty acids are only triggered by caloric deprivation plus the absence of insulin.
The trouble is, as we gain more weight from chronically eating carbohydrates combined with fats and proteins, we become more inundated by hunger signals that demand that we eat more often. Thus we are not able to get into the ketosis state of burning fats and, as a result, continue to gain weight and thus propagate the glycolysis cycle. Most people weigh their lowest when they are in young adulthood, just finishing high school or in college. Then they find out that, as they age, small amounts of weight are gained regularly and over time, which cannot be shed easily. Diets can create a temporary loss of weight but require tremendous will power and are not sustainable, as even short ‘binges’ caused by the body’s hunger mechanism can put all the weight back on as the body reverts to its most recent set point.
The ketogenic diet
One way to stimulate ketosis is with the ketogenic diet, a popular diet similar to the Atkins Diet but with emphasis on eating more fats in addition to restricting carbohydrates. On the ketogenic diet, carbohydrates are typically restricted to less than 50 per day, or less than 200 Kcal.
A common myth is that a low carbohydrate diet means a high protein diet, but this is not accurate. Protein, like carbohydrates, contains 4 Kcal per gramme, but there is a limit to the amount of protein we can process on a daily basis. Taking more than 200 grammes of protein (this is only 800 Kcal) can cause kidney and liver failure and is accompanied by exhaustion, vomiting, and diarrhea. While protein levels can be moderate, the bulk of calories on a ketogenic or Atkins diet comes from fats.
Many people find the ketogenic diet to be abundant and comfortable but may balk at its restrictions on food choices. For starters, foods containing sugars, honey, or sweeteners need to be eliminated. Fruits low in calories, like dragon fruit or small portions of apple, can be eaten, while higher calorie fruits like bananas, grapes, dates, and figs should be avoided. Vegetables cannot be of the starchy variety, so potatoes, pumpkin, and corn need to be eliminated, as do items like milk and yogurt that contain too much sugar from lactose and galactose. Complex carbohydrates such as rice, pasta, bread, cakes, crackers, and biscuits need to be strictly avoided.
The ketogenic diet, however, is abundant in animal fat (butter, cream, cheese, fatty meats) and non-starchy vegetables as this is needed for fiber. Nuts can also be eaten but need to be unsweetened. Unsaturated vegetable oils, besides olive oil, should be avoided as they contain too much Omega-6 fatty acids and not much Omega-3 fatty acids. Coconut oil is a saturated fat and can be consumed.
The benefit of the ketogenic diet is that it makes you feel fuller and less hungry, while being able to eat as much as you want to feel satiated and still be able to lose weight. However, to get into the ketosis state takes a few days of carbohydrate deprivation, during which people are often uncomfortable, tired, and irritable. These feelings pass once the ketosis state takes effect, but for many individuals, periodic carbohydrate cravings will still occur. In following this diet, one needs to maintain a strict regime since adding carbohydrates will normally result in a rapid weight gain and a return of feelings of hunger.
Intermittent fasting
Intermittent Fasting or IF has grown in popularity over the past few years. The design of the diet is to eat all the daily caloric requirements in an 8-12 hour window and abstain from eating the remainder of the day. There is less restriction on the dietary make-up of what type of calories are consumed. Some versions of IF involve eating only 500-800 Kcal twice a week, while eating as much as desired the remaining five days. The diet works because it also forces the body into ketosis simply by depleting the carbohydrate stores in the muscles and liver a few hours before the daily meal is taken, requiring the body to get energy from burning fat.
The main drawback is that the initial IF period is accompanied by tiredness, irritability, and difficulty concentrating. However, with several days of practice, the body gets used to the IF routine, and the level of difficulty becomes more manageable.
At the end of the day, all of these different diets are worth exploring to see if they can help manage your weight. In future articles, I’ll be writing more about other ways to shed pounds and maintain a healthy weight as well as other key areas that relate to maintaining health. Our bodies are fascinatingly complex pieces of machinery, so it’s important to learn about the key mechanisms needed for staying in optimum health and aging more gracefully with a higher quality of life.
Sudi Narasimhan is a seasoned healthcare executive, working in senior leadership roles in marketing, business development, operations, management and administration. He is a keen health enthusiast with a focus on exercise, nutrition, and the use of science to improve wellness and longevity. He is also the former senior director of Bumrungrad International Hospital in Bangkok.